
Participation in BPCI-A grew by 58% between March 2019 和 January 2020. 自愿退出期后3月, 其中16%的供应商退出了这个模型, 有1个,BPCI-A中还有295家供应商. 2019年夏天, CMS向新申请者开放了该模式, allowing them to join existing providers for the third model year, 1月1日开始, 2020. 根据CMS最新发布的与会者列表, 2,目前有41家供应商正在参与BPCI-A. Notably, only 18% of providers dropped from the model between MY2 和 MY3.

注意: There were 89 ACHs 和 150 physician group practices (PGPs) that dropped from the model between the start of MY2 和 the start of MY3.
供应商参与
The addition of 451 new PGPs reflects the growing trend of PGPs entering episode-of-care programs. Many commercial payers are putting physicians in the driver’s seat 和 incentivizing them to reduce utilization 和 increase care coordination through bundled payment programs. PGPs may sense that there will be increased pressure from commercial payers to participate in these models 和 are using BPCI-A (where losses are capped) as a trial run to gain the competencies needed to manage an episode of care.
1月1日起, 60% of PGPs were participating as a downstream episode initiator (EI), 这意味着他们的风险被控制在召集人层面. 在召集人结构下的参与不足为奇, given the resources conveners (either a third party or hospital partner) provide. 通常, the greatest barrier we hear about from physician groups regarding their readiness to manage bundled payments is access to meaningful analytics. 然而, we’ve found that once PGPs are exposed to the structure 和 reporting conveners provide, they are able to build their internal competencies 和 become confident managing on their own. It’s interesting to note that the percentage of PGPs participating as a non-convener actually increased from 20% in MY2 to 40% in MY3.


集选择
从历史上看, 在捆绑支付模式下, elective procedures have been more successful than medical; however, 脓毒症, 这是出了名的难以管理的状况, 现在是最受欢迎的一集吗, 由44%的供应商选择. The growth of 脓毒症 highlights the growing pressure hospitals are facing to develop internal programs to manage this condition. Many organizations find that the structure a bundled payment program provides helps inspire key stakeholders to work toward a common goal 和 hold them accountable for quality 和 financial outcomes.

心血管仍然是最受欢迎的bet8娱乐项目, accounting for about a third of selected clinical episodes. 在bet8娱乐范围内, the top three selected clinical episodes (cardiac arrthymia, AMI, 和, CHF) account for almost half (46%) of cardiac clinical episode selections. 然而, 心脏病发作的比例, 心律失常从MY2的20%下降到MY3的17%, 瑞郎从第二季的21%跌至第三季的13%. 这种下降并不令人意外, given our independent analysis of market data 和 conversations with clients. 在很多情况下, the investment needed to truly manage these patients outweighs the potential net payment reconciliation amount from CMS.

有趣的是, very few providers chose the four new MY3 episodes—seizure (3%), TAVR (1%), 减肥手术(1%), 和 inflammatory bowel disease (1%)—likely due to either the complexity of the episode or to the relatively low volume.
脊柱、骨骼和关节
Even though major joint replacement of the lower extremity (MJRLE)) is the only episode in Medicare bundled payment programs that has produced savings, MY3 marked a decline from 31% of providers to 22% of providers participating in a spine, 骨, 还有联合情节.
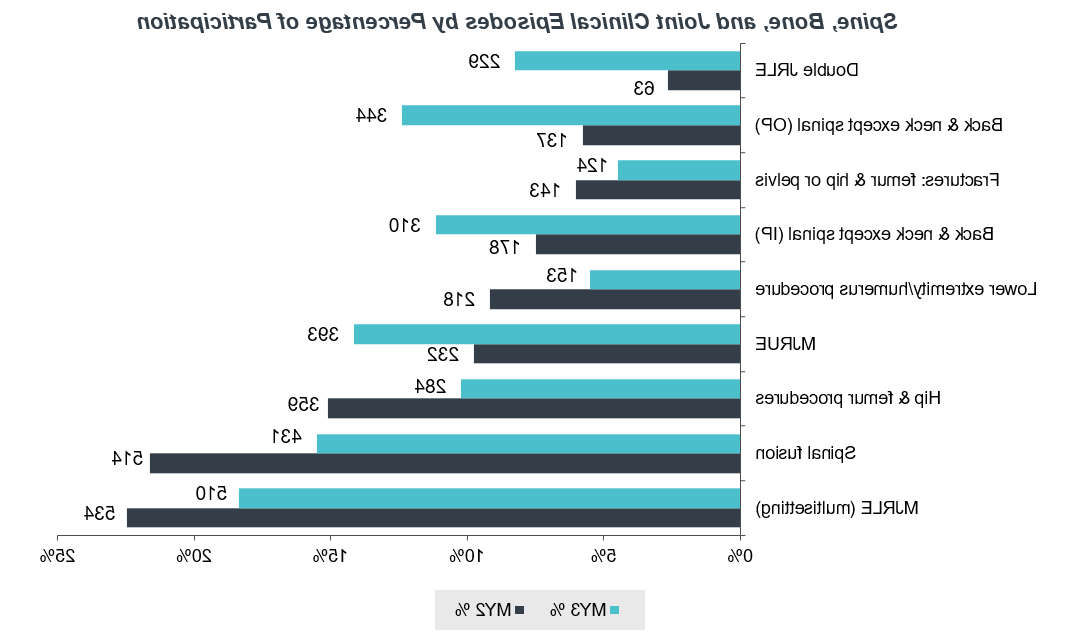
This marked decrease is largely the result of a CMS policy decision to change MJRLE from an inpatient (IP) episode to a multisetting episode to reflect the removal of total knee arthroplasty (TKA) procedures from Medicare’s Inpatient-Only List. In addition to exp和ing the criteria so that either an IP or outpatient (OP) TKA would trigger the episode, CMS还修订了目标定价方法, specifically adjusting baseline spending for IP TKA to mimic the supposed volume shift 和 impact of OP TKA clinical episode spending during MY3. 而从IP到OP的转变只会继续增长, 由商业支付者网站中立政策支持, many organizations are not quite ready to accept the risk of that shift. 在实践中, the shift from IP to OP has not happened as quickly as payers would like, 和 providers are worried that they will be penalized for not moving fast enough.

开始MY3, CMS has decided to pool the three spinal fusion episodes into a single spinal fusion episode. CMS hoped that this change would increase the number of hospitals eligible to initiate spinal fusion episodes 和 thus that more hospitals would choose the episode. 然而, 实际上,它导致了16%的参与率下降, indicating that the MY2 episodes were distinct enough that providers felt comfortable taking on risk only for select spinal fusion populations.

这对我的组织意味着什么?
The increase in providers participating in BPCI-A MY3 indicates continued interest in voluntary bundled payment programs. Further supporting this is the fact that a high number of providers who participated in the first two years of the model have remained in it. This trend suggests that both ACHs 和 PGPs can be successful with alternative payment models if the model is structured appropriately to reflect fair pricing methodologies. 如果你已经加入了BPCI-A, consider taking the next step 和 implement a commercial bundle (Bundled Payments in the Commercial Market: What You Need to Do to Be Prepared). If you are unsure that bundles are right for you, try taking our 基于价值的准备评估 看看你的组织下一步该怎么做.
2020年1月22日发布